Significant differences in the prevalence of SB between countries for the entire country sample were observed in 2002 (n = 15,363; χ2 = 791.963; DF = 28; p < 0.001), 2005 (n = 26,413; χ2 = 1990,145; DF = 54; p < 0.001), 2013 (n = 26,988; χ2 = 1744,015; DF = 52; p < 0.001) and 2017 (n = 27,240; χ2 = 1488,979; DF = 52; p < 0.001). Similarly, significant differences between countries were also observed for men in 2002 (n = 7082; χ2 = 381,420; DF = 28; p < 0.001), 2005 (n = 11,286; χ2 = 1111,757; DF = 54; p < 0.001), 2013 (n = 12,063; χ2 = 828,192; DF = 52; p < 0.001) and 2017 (n = 12,115; χ2 = 777,311; DF = 52; p < 0.001); and women in 2002 (n = 8281; χ2 = 441,942; DF = 28; p < 0.001), 2005 (n = 15,127; χ2 = 1057,698; DF = 54; p < 0.001), 2013 (n = 14,925; χ2 = 1005,487; DF = 52; p < 0.001) and 2017 (n = 15,125; χ2 = 79,778; DF = 52; p < 0.001). Descriptive characteristics of the sample can be found in Table 1.
Table 1 Descriptive characteristics of the sample
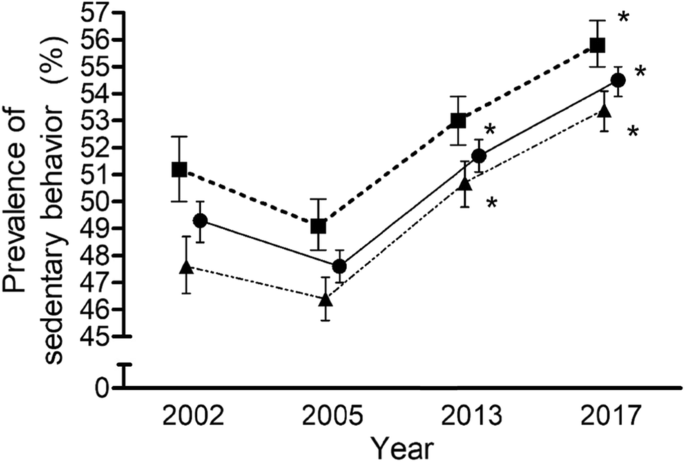
An association between the prevalence of SB and the years were found for the whole sample (n = 96,004; χ2 = 727,982; DF = 6; p < 0.001). These associations were also found for men (n = 42,546; χ2 = 307,233; DF = 6; p < 0.001) and women (n = 53,458; χ2 = 423,673; DF = 6; p < 0.001) separately. As is reflected in Fig. 1, over the 15 year-period in the EU member countries, the adjusted standardized residuals showed an increase in the prevalence observed versus the expected during 2013 and 2017 for the whole sample (adjusted standardized residuals = 2.9 and 13.1) and women (adjusted standardized residuals = 3.1 and 9.8), but only during 2017 for men (adjusted standardized residuals = 8.7). This trend was similar for each of the age groups analysed. Significant differences in the prevalence of SB between age groups for 2002 (χ2 = 179,189; DF = 10; p < 0.001), 2005 (χ2 = 289,434; DF = 10; p < 0.001), 2013 (χ2 = 184,806; DF = 10; p < 0.001) and 2017 (χ2 = 161,136; DF = 10; p < 0.001) were observed. The SB prevalence for 18–24 and 65 years and older age groups was higher than the expected for all years. Likewise, there were significant differences within age group between years (p < 0.001) (Table 2). However, SB prevalence was higher than the expected only for 2013 and 2017 in 35–44 age group, and 2017 in 45–54, 55–64 and 65 years and older age groups.
Table 2 Prevalence (%) of sedentary behaviour (>4h30min/day) in European Union (EU) countries adults between 2002 and 2017
In 2004, the number of EU countries increased from 15 to 28. Therefore, an additional analysis was performed only considering the first 15 countries. For this group of countries, an association between SB prevalence and the years were found for the whole sample (n = 60,325; χ2 = 661,052; DF = 6; p < 0.001). The analysis of the residuals showed an increase in the prevalence of SB observed versus the expected during 2013 and 2017 (adjusted standardised residuals = 4.5 and 12.3). These differences were also found for men (n = 28,060; χ2 = 333,673; DF = 6; p < 0.001) and women (n = 32,265; χ2 = 329,483; DF = 6; p < 0.001) separately. An increase was also reported in the prevalence of SB observed versus the expected during 2013 and 2017 for men (adjusted standardised residuals = 3.2 and 8.2) and women (adjusted standardised residuals = 3.1 and 9.0).
All the countries showed changes in SB prevalence between years (Table 2), with most of them showing an observed higher prevalence in 2017 than the expected (i.e., Austria, Belgium, Bulgaria, Estonia, France, Germany, Great Britain, Greece, Hungary, Italy, Ireland, Lithuania, Malta, Portugal, Romania, Slovakia, Slovenia, Sweden, and The Netherlands). Only Finland showed fewer observed cases than the expected for 2017.
While considering the subsamples of men and women separately for every country, and as can be observed in Table 3, similar patterns are generally reported. Differences between years were observed for most of the countries except for men in Croatia. The SB prevalence observed in 2017 was higher than the expected for men in Austria, Germany, Great Britain, Hungary, Ireland, Lithuania, Portugal, Romania, Slovakia, Sweden, and The Netherland. For women, the increase in the cases reported versus the expected was observed for Belgium, Bulgaria, France, Greece, Hungary, Italy, Ireland, Malta, Portugal, Romania, Slovenia, Sweden, and The Netherland.
Table 3 Prevalence (%) of sedentary behaviour (>4h30min/day) in men and women of European Union (EU) countries and gender differences between 2002 and 2017
When analysing gender differences (Table 3), SB prevalence in the overall EU sample was significantly higher in men compared to women for the whole sample. Almost all countries displayed greater SB prevalence in men in comparison with women over the years, with the following exceptions showing higher levels of SB prevalence in women in 2002 (Germany, Denmark, Ireland, and Spain), 2005 (Austria, Bulgaria, Estonia, Greece, Hungary, Latvia, Lithuania, Poland, and Slovakia), 2013 (Austria, Bulgaria, Estonia, Hungary, Latvia, Lithuania, Poland, Romania, and Sweden), and 2017 (Belgium, Bulgaria, Czech Republic, Estonia, Greece, Hungary, Italy, Latvia, Lithuania, Slovenia, and Sweden). Only five countries have shown a greater SB prevalence in women versus men for all the years (Bulgaria, Estonia, Hungary, Latvia, and Lithuania).
Comments